


Genomic medicine. Personalized medicine. Precision medicine.
When it comes to interpreting and applying big data in health care, people may not agree on the best terminology. Most agree on one thing: Big data is an abstract, intimidating concept.
DNA sequencing generates millions of data points for a single individual. Clinical trials yield massive amounts of treatment information. The electronic health record (EHR) expands with every patient encounter. And wearable fitness trackers and apps — which measure steps taken, food consumed, heart rate, blood pressure and sleep patterns, open up a whole new area of possibility.
Big data is coming at medical professionals from all directions. Many have no idea how to effectively leverage it for patient care.
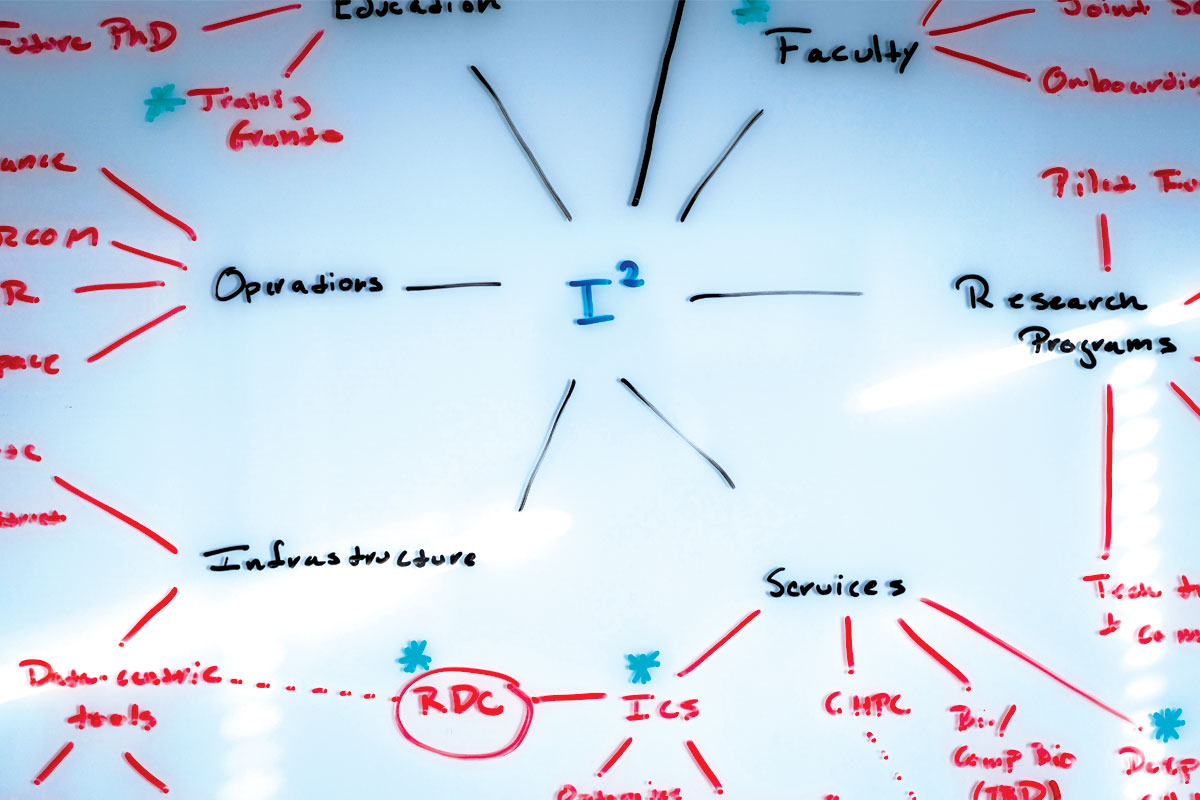
Philip R.O. Payne, PhD, is an internationally recognized leader in informatics, a field that translates big data into actionable knowledge. As inaugural director of the university’s Institute for Informatics, he leads the way he speaks — at double speed. In 20 months of existence, the institute has made significant inroads at this large, decentralized university.
For Payne, the path forward is clear.
“If you ask physicians what they want, it’s the equivalent of a ‘patients like mine’ button on their electronic device,” he said.
“They tell us, ‘Given the patient that’s in front of me right now, show me similar patients who have been seen in the past six months, one year or 10 years. What treatment decisions were made? Who had the best outcomes? Who didn’t?’
“Physicians want to know, based on their wisdom and the wisdom of colleagues, how to optimize outcomes for the patient in front of them.”
Information overload
Provider burnout nationally is at an all-time high, with doctors citing such factors as job complexity and having too few hours in the day. By some estimates, EHR upkeep requires 31 percent of physicians’ time.
A few decades ago, doctors could stay abreast of medical advances by reading scholarly journals. Now, it’s virtually impossible to keep up with the constant flow of information.
“Human short-term memory is optimized to remember seven pieces of information at a time, plus or minus two,” said Payne, also the Robert J. Terry Endowed Professor. “Informatics is essential to figuring out how we connect the dots between those millions of data points, contextualize them and deliver them back to clinicians who may have only 10 minutes with a patient to interpret and act on that information.”
Payne envisions a new landscape — where doctors and researchers have the necessary tools and expertise to extract meaningful information within vast data sets.
When many people hear the word informatics, Payne said, they associate it with interpreting the human genome, but that’s just one aspect of the institute’s work.
A top priority is improving EHR efficiency. The EHR requires a mental shift for some physicians who are used to free-form documentation of patient encounters on paper versus a more rigid, checkbox system that perhaps even influences medical thinking. Many clinicians find it clunky, burdensome and disruptive. Institute team members are shadowing clinicians at the point of care to design technologies that adapt to workflow.

Here, Andrew Michelson, MD, left, a pulmonary and critical care fellow, and
Sean Yu, a biomedical informatics doctoral student in the Payne-Lai lab, discuss analytical methods to predict septic shock.
Efficiently designed systems can close the gap between digesting the data and making clinical decisions, Payne said. “The real challenge is not getting more data. It’s figuring out what to do with what we already have.”
Recently, Payne and David H. Gutmann, MD, PhD, the Donald O. Schnuck Professor and director of the Neurofibromatosis (NF) Center at Washington University, employed informatics to predict symptom severity in children with NF1, a genetic disorder that causes brain and nerve tumors, as well as autism spectrum disorder (ASD). NF1 varies widely in severity and symptoms — from harmless brown spots on the skin and benign bumps to optic gliomas and malignant cancers. Parents don’t know which symptoms might manifest in their child.
In a matter of hours, using computer analytics and existing NF1 patient data, Gutmann and Payne improved risk models that others had created following months of painstaking deliberation in conference rooms. With even greater specificity, they outlined various NF1 subtypes, their trajectories and associations with optic gliomas and ASD.
This information allows families to plan ahead, and alerts clinicians as to whether additional imaging or other interventions are warranted.
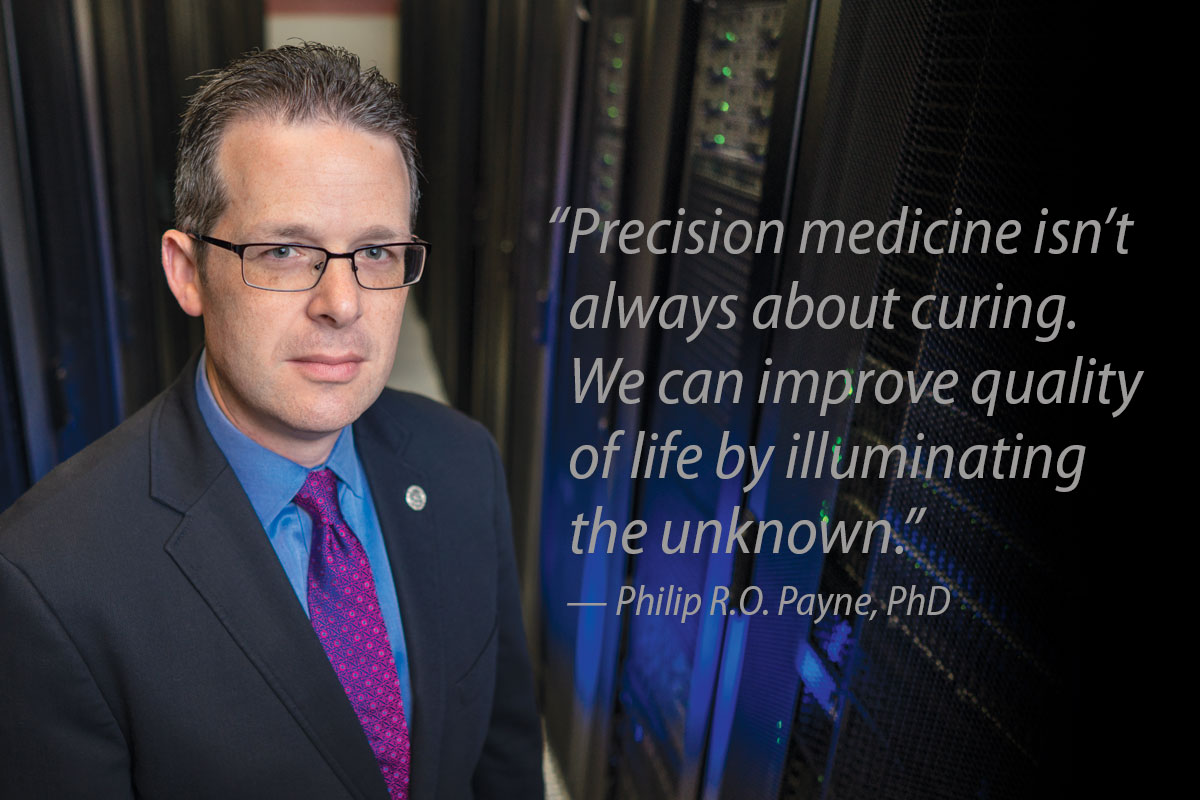
“Precision medicine isn’t always about curing,” Payne said. “We can improve quality of life by illuminating the unknown. It’s also helpful for the clinician in the exam room, who is facing imaging reports, EHR data, gene sequencing results, maybe a social/behavioral evaluation report — and an anxious child and an anxious parent. We are relying on physicians to integrate on demand and make the best possible decision. That’s a source of stress for providers, who have limited time and an EHR that isn’t designed very well.
“But if we can integrate that data and say to those providers, ‘This patient has an 80 percent probability of developing an optic glioma and here are the outcomes for the last 10 children you saw similar to this,’ then we’ve allowed them to get down to the really important information and have a conversation with the family and not just sit there clicking and pointing and typing.
“That’s the real promise if we do all the things we’re talking about.”
A data-driven approach, Payne said, is going to be a key differentiator as institutions compete to provide exceptional care in an information-rich era. Within its storehouses, big data holds the answers to pressing medical questions of our time; it has the power to develop drugs faster at lower cost, speed diagnosis, deliver on the promise of personalized, or precision, medicine, and improve quality of life.
A home advantage
Harnessing this power requires an environment that’s built to rapidly translate discovery out of the lab and into the clinic.
Washington University, in partnership with BJC HealthCare, stands uniquely poised to lead on the informatics frontier, with key strengths in medicine, basic science, cancer, genomics, radiology, public health, social work, business and engineering, among others. Nearby sits the 200-acre Cortex Innovation Community, a thriving hub for bioscience research, development and commercialization.
“We have one of the best genome institutes and one of the most productive and most impactful basic science research enterprises in the world,” Payne said. “We have some of the smartest care providers that you will meet. We have a unique living laboratory between Washington University Physicians and BJC HealthCare, where we have a large academic referral center, plus regional hospitals and primary care practice sites in urban and rural environments.
“We have all the pieces we need to study what the future of health care looks like. Very few U.S. academic health centers are truly primed to take advantage of the health-care information age.”
Until the institute’s launch, the university had all the raw pieces, except one. Although pockets of informatics strength existed — including leadership in the Human Genome Project, the Connectome Project and efforts to understand the microbiome — there was no central academic and professional home for informatics science and practice.
Every School of Medicine department chair contributed funding from department reserves to establish the Institute for Informatics, also known as I2.
One patient, one record
After putting critical team members in place, institute leaders turned their attention to their first, most fundamental task: Getting everyone within this expansive, 15-hospital system and medical school on the same page.
This June, with the institute’s active participation, the medical school and BJC HealthCare will roll out the Epic electronic health record system on the academic campus. It already has been launched in many of BJC HealthCare’s community hospitals. Once fully implemented, Epic will replace more than 50 standalone EHR systems that had been used by individual physician groups, specialty clinics, hospitals and even departments within the hospitals. Previously, outpatient data generated through Washington University Physicians (faculty practice plan) was not connected to hospital inpatient data. And some records were still paper-based.
As Sam Bhayani, MD, chief medical officer of Washington University Physicians, explains, the medical center draws patients who live hours away and who have complex problems and see multiple specialists.
Bringing data into one centralized location eliminates the need for patients to recall their entire medical history, such as the date of their last tetanus shot or prescription dosages, and will reduce treatment redundancies, potentially saving money, and help eliminate harmful drug interactions. It also allows clinicians to view patients holistically and consider all factors across the continuum of care. What should emerge is a more comprehensive picture of a person’s health care, including total cost of care.
This, however, is only half of the vision. Patient information must be returned back to investigators as they consider new ways to solve complex health-care problems. Data mining within a decentralized system has been an arduous, inefficient task.
“For some patients, we had very little data. All we knew is what happened during their hospital stay,” said Chief Research Information Officer Albert M. Lai, PhD. “If you’re a researcher trying to understand optimal care delivery, it’s basically impossible given this fragmented view.”
A new research paradigm
A centralized EHR has revolutionary research implications for Washington University — joining together and unlocking access to more than 6 million records of inpatient and outpatient care.
“We want to translate data into knowledge,” Payne said. “We want to create a system where what we learn from each patient informs how we treat other patients and what questions we ask in the lab. In turn, we want what we learn in the lab to benefit patients more quickly.
“Right now, we have clinical investigators seeing patients. But they go back to their labs and they don’t have access to the data generated by their own patients, at least not to the degree necessary to test basic hypotheses. We need to make that data more accessible.”
The real forward leaps in innovation will come as the institute builds out a large, integrated database — known as the Research Data Core (RDC) — that links all data. The RDC powerhouse will include the common EHR, which feeds a continuously updated stream of patient data, plus data from any remaining legacy or departmental clinical systems. Plans call for the addition of genomic and biospecimen information.
Statistical data analysts within the institute will manage the RDC. These informatics professionals will help researchers pull data from the central system, design studies and maintain patient confidentiality. They and other team members are available to educate, answer questions and analyze and visualize data in meaningful ways.
Through self-service tools, researchers will be able to access the RDC and do some analysis at their own computers. Informatics leaders say a new partnership with a company called MDClone also has the potential to fast-track research. Washington University is the first U.S. academic institution to have this technology.
Under current federal regulations, investigators must wait weeks or months to begin research projects involving real patients. For each project, researchers must file paperwork and wait for approval from an institutional review board (IRB), an administrative body that protects the rights and welfare of human research subjects. Following approval, researchers then must wait for a data analyst to pull the necessary data before research can get underway.
MDClone’s unique niche is its ability to create synthetic data — data that looks like an actual patient population, but isn’t. Data engines yield synthetic data that is statistically identical to original protected health information, but without privacy concerns.
“With MDClone, you could effectively have no time delay,” Lai said. “If you think of an idea, you can pull up the data and analyze it, right then and there, from the computer in your office, potentially make discoveries on the data, with zero risk to patient privacy.”
If the data looks promising, researchers can follow the standard IRB steps to confirm the result with real data. If not, Lai said, they can just move on to the next question.
The institute is testing MDClone’s performance via pilot research projects. Pending a successful evaluation, MDClone will become part of the RDC infrastructure.
Creating efficiencies in research saves time and allows grant dollars to stretch farther, Payne said, which, in turn, will attract top U.S. researchers.


Speeding discovery
Payne hopes to speed up the process of taking discoveries into clinical trials. Currently, it can take 15 to 20 years and more than $1 billion to develop therapeutic agents for disease.
Treatment solutions, however, are waiting to be found in big data. Repurposing or using new combinations of approved drugs, which already have passed toxicity tests, could save valuable time.
Using an informatics concept known as “machine learning,” computers can be programmed to comb through clinical and drug data, going back through decades of medical literature, analyzing billions of variables, to discover meaningful patterns and new uses for existing medicines.
Payne, also a cancer researcher, points to malignant melanoma as one example. Frontline therapies are effective at causing tumors to disappear, but patients often become resistant within 12 months of the first treatment. By using public data and computational methods, researchers have found drugs — developed for other diseases — that could be combined with melanoma frontline therapies to prevent or delay resistance onset. So far, Payne’s research team has taken this combination therapy all the way to animal models, and they did it in about a year.
Once a therapeutic agent is ready to move to clinical trials, the RDC also should make it quicker and more efficient to identify test subjects.
Enhancing human health
The dream, Payne said, is to use big data not only to help the sick, but also to keep people well, to intervene in the communities where they live, work and play, and not just inside our hospitals.
An evolving EHR likely will include more data about patients’ daily activity levels, gathered through smartphones and fitness trackers, and other health influencers, such as water quality in the home, proximity to grocery stores and family support networks.
Big data has the power to promote wellness by generating a picture of the whole patient — connecting genes and environmental factors to social factors and outcomes.
“The institutions that figure out how to bring all these pieces together will be the first to begin delivering personalized, precision medicine,” Payne said. “Rather than treating people as a function of averages, personalized health care that is powered by big data is about enabling physicians to provide the right care at the right time, based on the unique characteristics of the patient in front of them.”

Launching the institute
When Philip R.O. Payne, PhD, previously chair of the Department of Biomedical Informatics at The Ohio State University, signed on to become the institute’s founding director, he brought longtime colleagues with him.
This allowed for rapid deployment in targeted areas:
- Speeding pace of discovery out of the lab into human studies
- Building systems that improve how physicians treat patients
- Using data to improve health of communities
Most faculty affiliated with the institute, which is housed in the Division of General Medical Sciences, will hold dual appointments in other departments and schools. This is part of a strategy to extend the institute’s reach across the university. An informatics expert embedded in anesthesiology or pediatrics, for example, will collaborate on projects related to these subjects.
Key informatics faculty investigators

Clinical research informatics
Chief Research Information Officer Albert M. Lai, PhD, an expert in informatics infrastructure who specializes in solving problems in the clinical domain. He oversees a core services team of programmer analysts, software engineers, database administrators, data analysts and bioinformaticists.

Population health informatics
Randi Foraker, PhD, MA, FAHA, who applies informatics techniques to solve problems in the population health domain. She also serves in the Institute for Public Health.

Applied clinical informatics
Po-Yin Yen, PhD, RN, an assistant professor at the Goldfarb School of Nursing at Barnes- Jewish College, who works with frontline caregivers to understand daily workflow and improve health information technology.
Published in the Summer 2018 issue